


The 5th Spine Surgery Master Class – 2025
January 2, 2025
Spine Master Class Batch 5th in Conjunction with World Endoscopic Spine Society (WESS) Congress 2025
January 6, 2025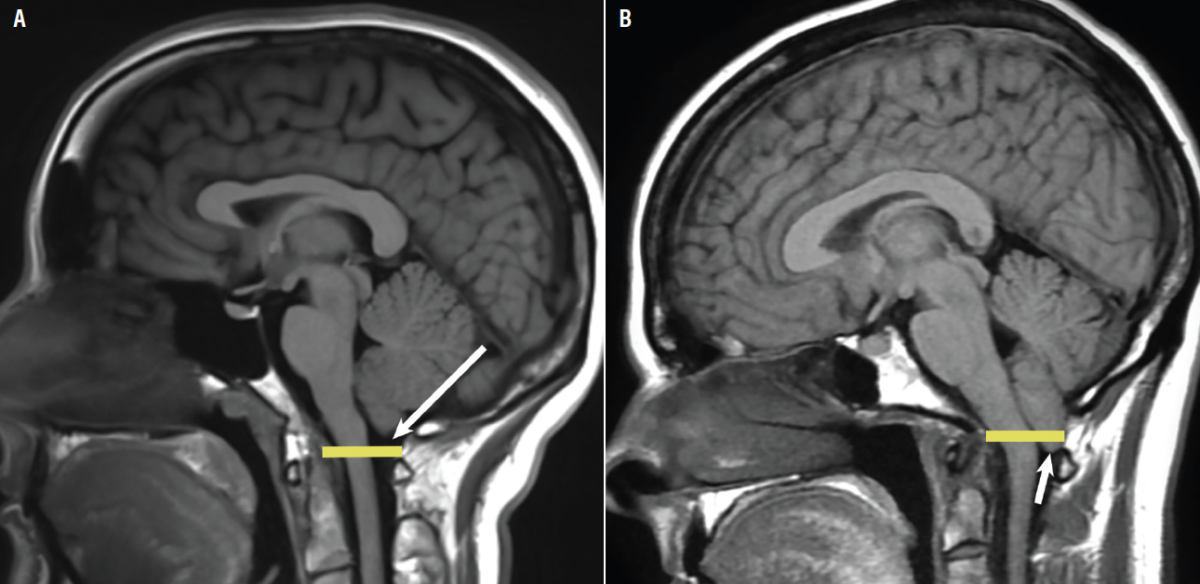
Paper Written by :
Rully Hanafi Dahlan. Sevline Estethia Ompusunggu. Lukas Galileo Malau
Division of Neurospine, Peripheral and Pain
Department of Neurosurgery. Faculty of Medicine Padjadjaran University
Adventist Hospital
Bandung – Indonesia
Chiari malformation, is the name to describe a group of deformities of the hindbrain (cerebellum, pons and medulla oblongata). Problem range from herniation of the posterior fossa contents outside of the cranial cavity to absence of the cerebellum with or without other associated intracranial or extracranial defects such as hydrocephalus, syrinx or spinal dysraphism. Its Classification based on the morphology of the malformations as evidenced radiologically or at autopsy. Chiari I: Greater than 5-mm descent of the caudal tip of cerebellar tonsils past the foramen magnum. Chiari II: Brainstem, fourth ventricle, and greater than 5-mm descent of the caudal tip of cerebellar tonsils past the foramen magnum with spina bifida. Chiari III: Herniation of the cerebellum with or without the brainstem through a posterior encephalocele. Chiari IV: Cerebellar hypoplasia or aplasia with normal posterior fossa and no hindbrain herniation. There are multiple proposed theories including molecular, hydrodynamic, and mechanical. Genetic syndromes related or more commonly idiopathic reduced volume of the posterior fossa leads to a displacement of the cerebellar tonsils into the spinal canal. Other type have invariably results in the setting of myelomeningocele. Leakage of cerebrospinal fluid (CSF) to the myelomeningocele yields herniation of the hindbrain into the spinal canal, which disturbs the cerebrospinal fluid normal flow and subarachnoid adhesions.
Chiari malformation is type 1 is the most common type and occurs in approximately 1 in 1000 births. There is a slight female predominance of cases (1.3 to 1). Type 2 malformation is associated with neural tube defects, especially myelomeningocele, in almost all cases. Neurologic signs and symptoms can arise from 2 mechanisms. First, Direct compression of neurological structures against the surrounding foramen magnum and spinal canal Syringomyelia or syringobulbia development . The obstruction of cerebrospinal fluid (CSF) outflow eventually results in syrinx development Fluid-filled cavities (syrinx) develop within the spinal cord or brainstem, resulting in neurologic symptoms as the cavity expands.
When we talk about Chiari type I malformation the most common presentation is suboccipital headaches and or neck pain (80%). Symptoms are exacerbated when asked to perform the Valsalva maneuver. Other common presentations include ocular disturbances, otoneurologic symptoms (dizziness, hearing loss, vertigo), gait ataxia, and generalized fatigue. Myelopathy classically presents with dissociated sensory loss. Cerebellar signs, including ataxia, dysmetria, and Nystagmus, lower cranial nerve deficits (IX, X, XI, XII CN) either from direct compression of the cerebellum or medulla at the foramen magnum or from syringomyelia or syringobulbia.
It is not an uncommon scenario to find patients with radiological findings compatible with Chiari malformation with no clinical manifestations of the disease (incidental Chiari malformation). Therefore, unspecific symptoms such as generalized fatigue or classic pattern migraines are not necessarily related to the Chiari malformation.
The main treatment for Chiari malformation is surgical with the goal of re-establishing the CSF flow across the craniovertebral junction and decompressing the nervous system elements, and who have no symptoms can be managed medically. Headaches and low neck pain can be treated with muscle relaxants, NSAIDs, and temporary use of a cervical collar. Surgery is recommended for patients complaining of the classic pattern of symptoms and confirmed tonsillar herniation. In the setting of tonsillar herniation without clinical manifestations, observation is recommended, surgery is recommended if symptoms develop. Surgical options including bone craniectomy, posterior fossa decompression, dural opening with or without duroplasty, syringe shunting (diversion), resection of membrane atlantooccipital and foramen magnum opening. The result, somehow still in wide variation, and the treatment surgical option for chiari malformation still in debate, and become one of the most controversies in world of Neurosurgery
Keywords : Chiari, posterior fossa decompression, duroplasty
